Injury Prevention and Public Education
Injury prevention/public education programs begin with the collection and analysis of population and patient data from a wide variety of sources to describe the status of injury morbidity, mortality and distribution throughout the state. Injury epidemiology is concerned with the evaluation of the frequency, rates and pattern of injury events in a population and is obtained by analyzing data from sources such as death records, hospital discharge databases and data from EMS, Emergency Departments and trauma registries. Trauma systems must develop strategies that help prevent injury as part of an integrated, coordinated and inclusive trauma system. For years, the IDOH has conducted an array of injury prevention programs. With the creation of the IDOH Trauma and Injury Prevention Division in 2011, we have shifted our focus from injury prevention programming to the collection and analysis of injury data (epidemiology) and recognized best practices in the injury field, which we can push out to those around the state conducting impressive and far-reaching injury prevention programming. The IDHS and other Indiana state agencies also conduct injury prevention/education activities.
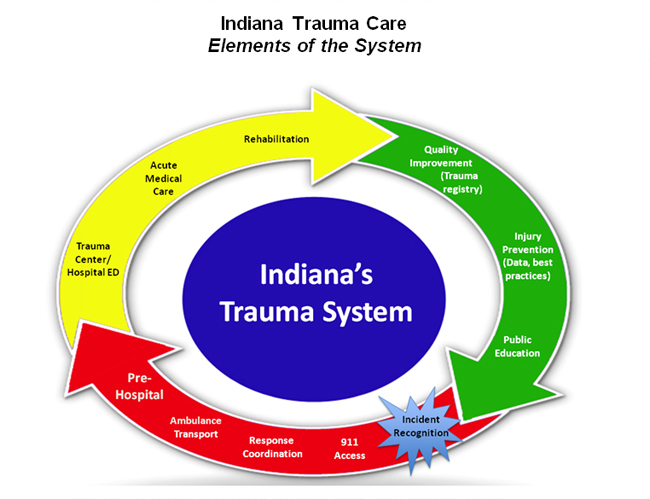
Pre-Hospital
The first phase of Indiana’s trauma system activates immediately following an injury — a call is made to the 911 operator, the response is coordinated among various Emergency Medical Services (EMS) ambulances, initial assessments and diagnoses of the patient are made, and the patient is stabilized and quickly but safely transported to a local hospital or trauma center. EMS crews are often the critical link between the injury-producing event and definitive care at a trauma center or local hospital. The first hour post-injury is known as “the Golden Hour,” when critical skilled care must be provided. The Indiana Department of Homeland Security (IDHS) is responsible for oversight of the EMS in Indiana.
Trauma Center/Emergency Department
Trauma centers are hospitals that have applied for, and been granted, verification as a trauma center by the American College of Surgeons (Levels I, II and III, with Level I trauma centers providing the highest level of trauma care). Trauma centers are unique in their capabilities and are NOT the typical community hospital Emergency Department. But for all the trauma centers we have, there are not enough of them to adequately meet the needs of Hoosiers and visitors to the state who become injured. Hospital Emergency Departments are part of the statewide trauma system, as not all injured patients are taken to trauma centers; the vast majority of injured patients can be, and are, treated at local, non-trauma center hospitals. Non-trauma center hospitals stabilize and provide definitive life-saving care for patients who don’t require trauma center care. Many times, especially in rural areas where timely access to trauma centers is not possible, non-trauma center hospital Emergency Departments provide definitive care to trauma patients out of necessity.
Acute Medical Care
Acute medical care facilities are hospitals that provide care for short periods of time. Trauma patients are admitted to an acute medical care facility in order to allow them to recover from their injuries as well as recover from procedures and surgeries utilized to fix their injuries. The most serious injuries will have the patient recovering in the intensive care unit, while less seriously injured patients may recover in a critical care unit, a step-down care unit or a medical-surgical care unit. There are more than 120 hospitals in Indiana, all of which are regulated by the ISDH.
Rehabilitation
Rehabilitation centers care for trauma patients post-acute care and seek to enable these patients to realize their fullest post-injury potential. Oftentimes, these patients have sustained severe or catastrophic injuries, resulting in long-standing or permanent impairments. Rehabilitative interventions strive to allow the patient to return to the highest level of function, reducing disability and avoiding handicap whenever possible. When rehabilitation results in independent patient function, there is a 90 percent cost savings compared with costs for custodial care and repeated hospitalizations. Unfortunately, the rehabilitation phase of care often isn’t sufficiently integrated into the trauma system, even in the most mature, well-developed statewide trauma systems.
Quality Improvement (Trauma Registry)
A state’s trauma registry is not only the repository for data about trauma in its state, but it exists to improve outcomes for injured patients. The registry uses data to measure and analyze all aspects of the system to ensure the highest quality care is provided to all. The IDOH operates the Indiana Trauma Registry and is responsible for instituting processes to evaluate the performance of all aspects of the system, from the EMS provider to the trauma center/acute care hospital and the rehabilitation provider. The IDOH Trauma Registry has been operational since 2008.